Rule out criteria have many benefits, but they are not perfect. Sometimes, they can miss an important disease process or problem. Those who provide care to patients must use them wisely. In this post, the discussion is aimed to help explain the purpose of rule out criteria as well as their pearls and pitfalls.
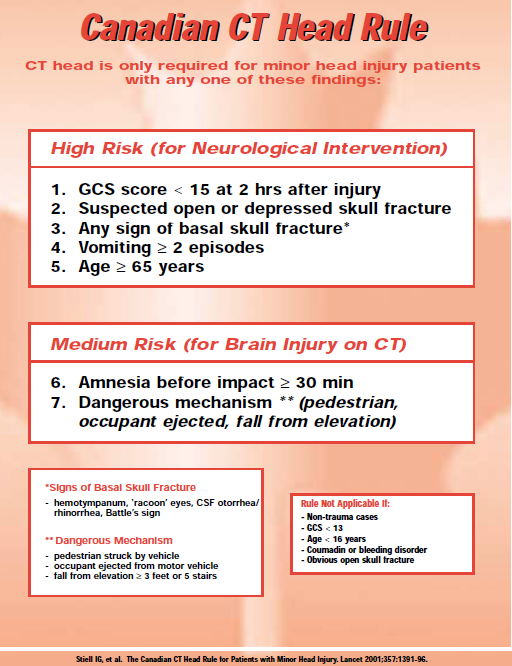
Imagine a 36 year old male friend was playing softball when he got hit in the head by a softball that was thrown at him. He did not lose consciousness and he has been acting his usual self. In fact, he remembers everything and wants to go back to the game. He has no headache, no vomiting, no bruising, and no signs of broken bones to the head or face. The coach says he needs to get checked out and goes to the closest emergency department (ED). As the Canadian CT Head Rule graphic from The SGEM shows above, the patient described in the podcast would not have been caught by the criteria even though he was found later to have two important brain bleeds. This does not mean though that all head injuries need an expensive CT that carries with it a risk of cancer from the radiation. Rather, that patient was the exception to the rule.
Rule out criteria are not meant to be perfect. Rather, they are meant to help risk stratify patients. As stated above, not everyone needs a head CT. Most will be fine and no bleeding would be found even if such as CT was performed. However, to expose someone to a head CT unnecessarily exposes them to radiation that in turn increases their risk for cancer. By using rule out criteria and other clinical decision aids, those who provide care (including the ED provider) can help decide if a patient is in need of further testing. These tools are used in a number of conditions. Some of the most common are for head injuries (there are ones both for children and for adults), neck injuries, blood clots in the legs and clots in the lungs, risk for sepsis, and risk for heart attacks. Let us talk briefly about the last example, heart attacks. Although rare, the clinician taking care of you may decide you still need to be in the hospital even if your HEART score is low for a potential heart attack. The criteria itself may not score high enough if you have obvious EKG changes or high blood levels for a heart attack. Thus, such criteria are only one piece of the puzzle. Although not all providers will discuss their use of rule out criteria in detail, they may mention the risk stratification portion. This part is to help explain the risks and benefits of the tool being used. They may discuss how the tool is not perfect and that some cases may be missed. However, sometimes that miss rate is considered acceptable due to the risks of potential complications with the additional testing or inappropriate treatment. Although we may want to get the testing for our own benefit (either the benefit of the patient or the provider), a serious discussion or at least consideration of the risks must be evaluated in detail. The tests and treatments for blood clots for example can be life-threatening. Smaller, less important clots in the lungs are less likely to have a negative impact compared to the treatment chosen. In conversation, a provider may mention odds ratios or percentages. These numbers are meant to give an idea as to these risks. Sometimes by going step by step with the different factors, a discussion can be had to make sure that the risk group is appropriate. In general though, rule out criteria are meant to help reduce the need for unnecessary testing while still keeping patients safe and reducing their risk to a bad outcome such as death or disability. The important thing to remember though is that no tool or provider is perfect and there is always a risk with any method to evaluating and treating patients. If you are interested in more information about rule out criteria along with their pearls and pitfalls, consider seeing the podcast post under the Emergency Professionals side of the website. This is also the same area to find the sources that were used to cover the information provided. Remember to look us up on Libsyn, share on Facebook, retweet on Twitter, and rate on iTunes to help spread the word on TOTAL EM. If you have any questions you can comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Future UpdatesThe current main focus is on further developing the Emergency Professionals side but keep checking as more updates are coming very soon! Archives
November 2017
Categories |
||
 RSS Feed
RSS Feed