Patients often come in complaining of a possible spider bite, but is this actually the cause of their symptoms? In this blog and podcast, we talk specifically about brown recluse bites, differentiating them from other causes, treatment, and other pearls.
Staph infections, especially MRSA, are often thought by patients to be brown recluse bites when in fact these bites are very uncommon. Indeed, prior evidence has demonstrated that the likelihood of MRSA is significantly increased if a patient says they have a spider bite but did not see a spider or feel its bite. This time we discuss how to recognize and manage brown recluse bites.
Brown recluse spiders are most abundant and active at night during the warm months, are non-aggressive, reclusive, and prefer to retreat when threatened. Brown recluse spiders measure 2-3 cm from leg to leg, have 6 eyes arranged in 3 pairs (most spiders have 4 pairs), and has a characteristic dark, violin-shaped spot on the dorsal aspect of the cephalothorax. Envenomation can result in dermonecrosis and, less commonly, a potentially fatal systemic illness that includes hemolysis with DIC, thrombocytopenia, proteinuria, and rhabdomyolysis, with subsequent renal failure. Death in the United States is extremely rare. The venom contains cytotoxic, proteolytic, coagulopathic, and hemolytic components. The primary toxic component is sphingomyelinase D, which is largely responsible for necrosis and hemolysis. Hyaluronidase causes the characteristic gravitational spread of the lesion. Brown spider bites typically occur during dressing or sleeping when spiders become trapped in clothing or bed linens. The bite can produce a sharp, stinging sensation, although frequently the victim is unaware of having been bitten. Over time, the wound typically develops an erythematous halo surrounding a central hemorrhagic vesicle. Occasionally, the central vesicle will be surrounded by an area of ecchymosis, surrounded by a ring of pallor and an outer ring of redness. As early as 24 hours after envenomation, fever, arthralgias, nausea, vomiting, diarrhea, rash, myalgias, and headache can develop. By day 3 or 4, the hemorrhagic vesicle becomes necrotic, and an eschar forms. After 2-5 weeks, the eschar sloughs, leaving an ulcer that often heals by secondary intention, though some may require skin grafting. In severe cases, there can be progressive tissue necrosis that is particularly severe in fatty regions such as the buttocks or thighs. Below is an example of wound progression in a 10 year old girl in New Mexico. 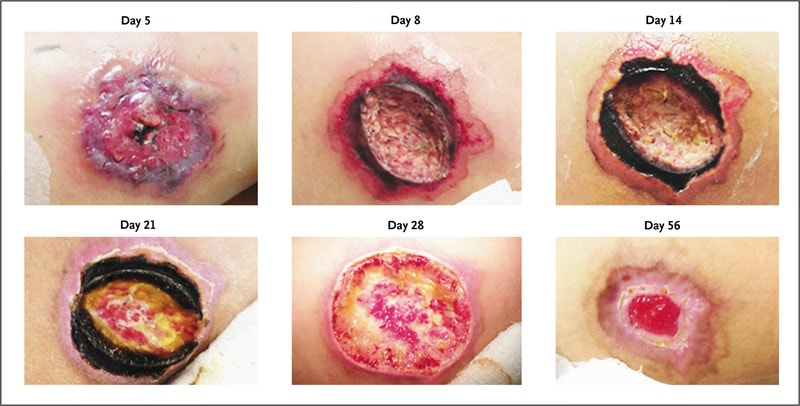
Diagnostic Pearls
Severe burning, pain, and pruritus at the bite site within 2-6 hours is characteristic of a brown recluse envenomation. The mnemonic "NOT RECLUSE" lists the features of look-alike conditions. The presence of each makes the diagnosis of brown recluse spider bite unlikely:
First aid treatment includes:
This was a great review and several sources were used. However one of the best sites that did a very good job with summarizing the information (as well as having additional details) is VisualDx which is a paid service but well worth it if you need to learn more about dermatology. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
2 Comments
11/10/2023 10:41:36 am
This morning, my brother said he saw a scary-looking spider in his attic. He bought an old house that's been sitting without anyone living in it for years, so he's cleaning and renovating it. I'm worried that he'd be dealing with a brown recluse spider and get bitten by one, so I'll recommend he reads your intake to see if it's the same spider species. Thanks for explaining that a brown recluse spider bite leads to dermonecrosis. Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed