
Now that our month of point of care ultrasound (POCUS) is over, it is time to talk about other clinically relevant topics. Michelle Perkins is back again this time to help us cover tickborne illnesses in the United States.
Introduction
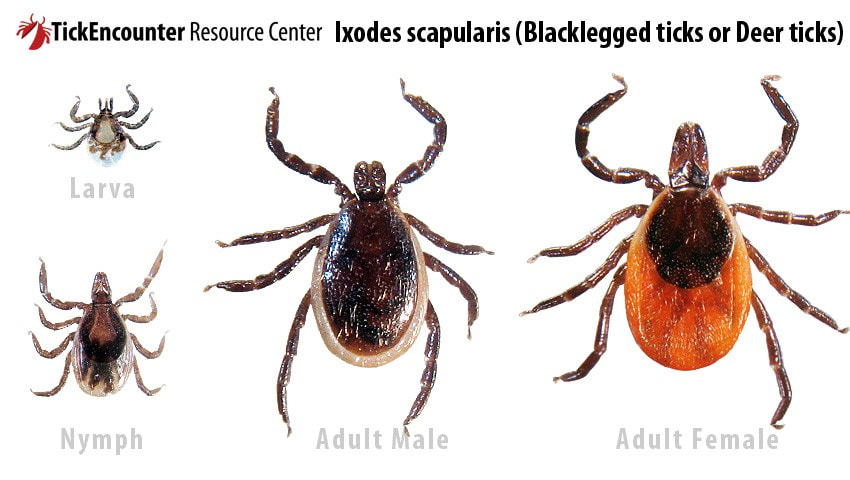
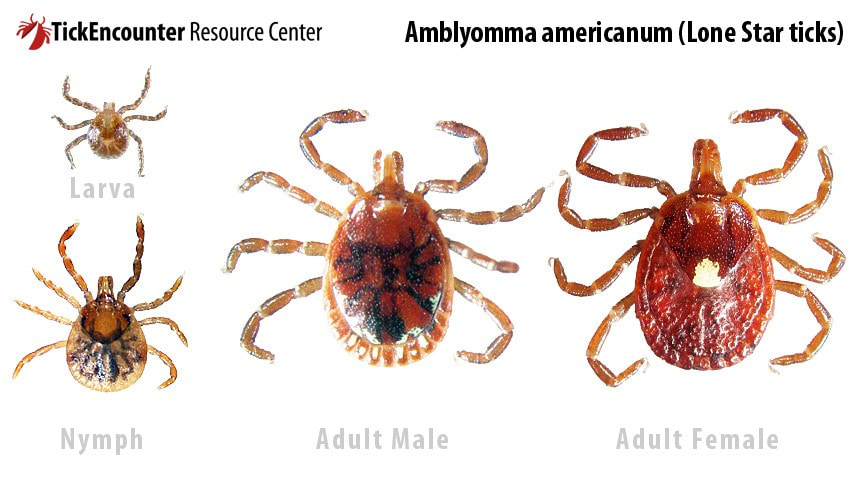
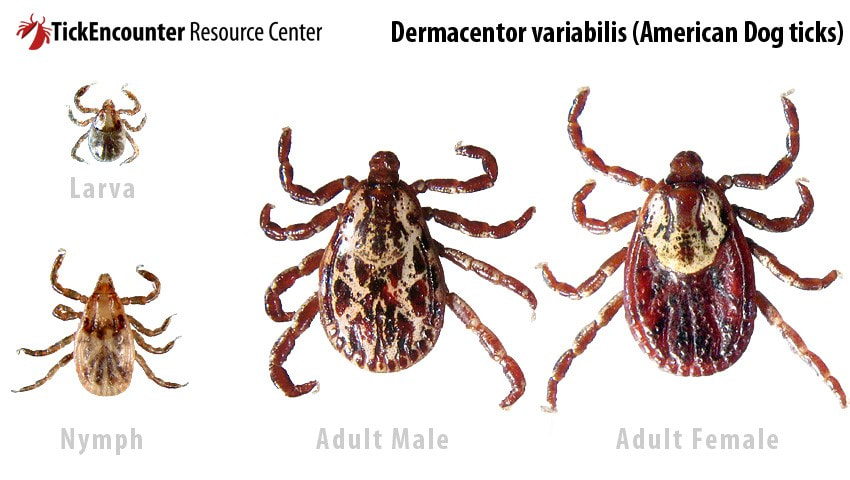
Tick Talk
General Workup and Diagnosis
Anaplasmosis
Ehrlichiosis
Babesiosis
Lyme Disease

Disseminated illness: all bets are off. This is where you see the weird stuff. You can see multiple bullseyes, flu symptoms, and rheumatologic manifestations like migratory joint pain, muscle pain, and bone pain. You can see cardiac manifestations, like AV nodal block, myocarditis, and pericarditis. And the neuro stuff can be deceptive—you can see meningitis or even encephalitis, you can see neuropathy, Bell’s palsy, and/or cognitive issues. As far as labwork, you may see an elevated ESR/WBC, but generally not much acutely. Lyme serology is negative for the first few weeks, so not helpful in that window. You also can’t distinguish between active and past infection with serology. So you can’t use testing to measure treatment response.
RANT TIME
Rocky Mountain Spotted Fever

Tularemia
Alpha-gal Reaction
Summary
Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed