
It is that time of year. It is cold and croup is in the air. There is a spectrum of patients that present ranging from the mild to the life threatening. We discuss how to manage these patients.
Croup is a viral infection most commonly caused by parainfluenza types 1 and 3 but other causes include influenza A and B, adenovirus, respiratory syncytial virus (RSV), and metapneumovirus. The resulting generalized airway inflammation and edema of the upper airway mucosa causes one of the most common upper airway obstructions in young children. Significant complications though such as endotracheal intubation and death is rare.
Classically, patients are between 6 months and 3 years of age with a sudden onset of a barky cough, inspiratory stridor, hoarseness, and respiratory distress that is worse at night. The barking cough usually disappears after 48 hours and often lasts only 3-7 days. A Canadian paper outlines some of the key differential diagnoses which we included as a table below along with adding the importance of recognizing retropharyngeal, parapharyngeal, and peritonsilar abscesses. 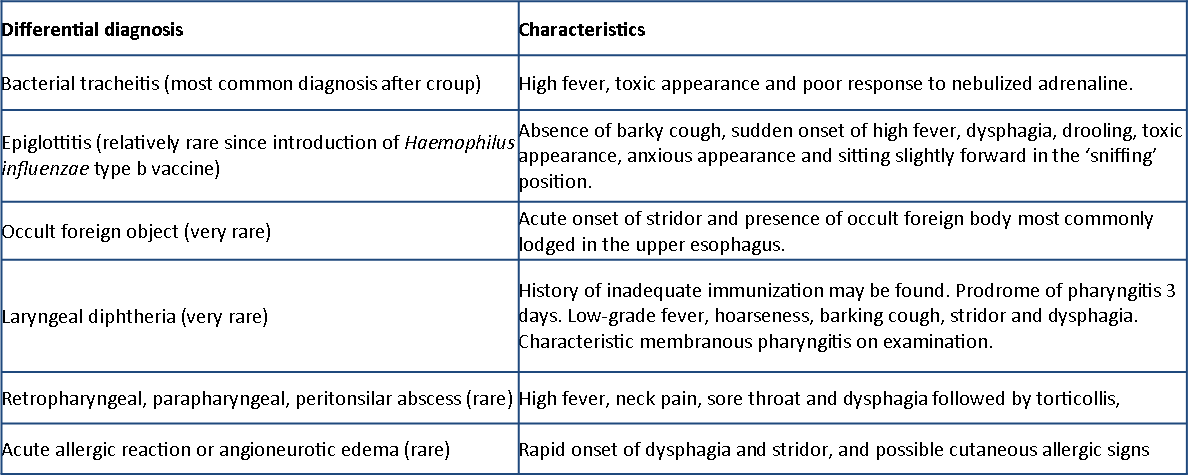
Recently, the Canadian Paediatric Society published a paper which a great algorithm breaking down the approach to a patient with croup. Essentially, the care depends highly on the severity of symptoms. This is generally a less is more approach. Special care should be taken to avoid frightening the patient.
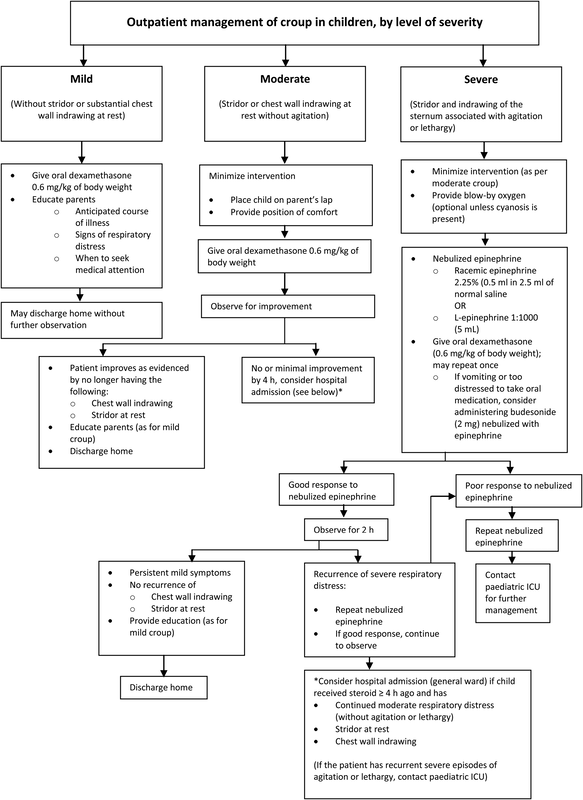
Dexamethasone is generally given at 0.6mg/kg, but some trials have used lower doses without clear evidence of benefit. Using dexamethasone can help reduce return visits and admissions, have improved sleep, and less stress to the parents.
Nebulized epinephrine (usually racemic) is safe, effective, and fast acting. The effects can be within 10 minutes and disappear after 2 hours. Safe discharge can be done in 2-4 hours. Other therapies do exist, but their evidence such as with heliox is limited. Children who fail the initial measures may require pediatric ICU admission. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed