
This one is sure to generate some controversy, especially by my fellow #FOAMed colleagues but it is a conversation we need to have in all earnest. We must seriously consider if double sequential defibrillation (DSD) is as good a plan as we may have originally thought.
Before we dive into the subject at hand, check out Yes, I Scan at AAPA May 2019. For students this is free but there will also be paid workshops in conjunction with SPOCUS and Practical POCUS. There are also paid sessions for a VERY low cost and you can register now for discounted rates to the conference.
Immediately when coming up with this idea for a topic, Jeff Goldblum's line from Jurassic Park came to mind, "You're scientists were so preoccupied with whether or not they could they didn't stop to think if they should." We in the #FOAMed world get very excited for innovative ideas, but sometimes it is to our own downfall. With that said, that is not to mean that DSD or any other clever advancement is a bad idea, but it should at least give us pause.
There have been a multitude of previous #FOAMed discussions on this topic with some favorites including posts made by The Resus Room, briefly on EMCrit (but there is a free video from EM:RAP), and REBEL EM where there have been multiple posts on the subject. As discussed by Salim Rezaie and others well, this is meant to be a last ditch effort. However, some have advocated for earlier placement. Once concept is the use of original pad placement for three times (often anterior/posterior), then switching to the other routine method (anterior and lateral placement) for another two shocks while keeping the original pads in place. If both single pad sets fail, both sets of pads are in good position for DSD to be performed.
The main concept of the technique is that it is meant for those with refractory ventricular fibrillation in which multiple attempts have already been made with the usual approach to defibrillation. Other therapies may have been attempted such as esmolol. Finally, an attempt may be made by placing two defibrillators to encourage defibrillation. The general concept on a physics level is that there will be two directions of energy that flows through the heart in a near (unlikely literal) simultaneous time-frame to cover more of the myocardium and encourage cardioversion. There is not strong research on the placement, but REBEL EM illustrated the main options well. 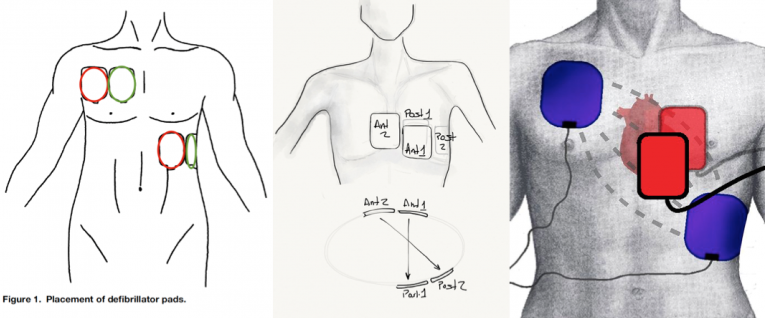
There have been case reports and case series supporting its use. Given its rarity, it is hard to find higher quality data. A retrospective case study by Ross et al in 2016 in the journal of Resuscitation failed to find a statistically significant difference in neurologically intact survival between the dual defibrillation group (6%) and standard defibrillation group (11.4%). Although it is worth noting that bystander CPR in the DSD group was 30% vs 45% in the standard defibrillation cohort and witnessed arrest in the DSD group was 38% vs 54.6% in the standard defibrillation cohort, the data should still be considered an important point as it was a much larger data set than the positives. We must also remember that case reports are inherently biased as they are designed to report the positives (such as successful DSD) versus the less desirable and often unpublished negative results including when there are negative effects (such as broken or failed equipment). More recent evidence in Resuscitation in 2017 by Emmerson et al focused on patients in London with refractory ventricular fibrillation. Again, the evidence was lacking to demonstrate a clear benefit. Both of these retrospective studies were made into a meta-analysis published in 2018 in Resuscitation which reflected the negative findings.
Why does this matter though? Why did Jurassic Park come to mind when thinking about this topic. It is because many of us have not spent time thinking if we should be performing this procedure. DSD is off-label and thus not FDA approved. We of course perform other procedures with devices in a non-approved fashion, but most are not at the risk of damaging the machines. Importantly, if the machine is damaged this may result in failure to save the next patient. We know that early defibrillation is a key component to survival to hospital discharge neurologically intact and having a damaged machine directly impacts care of the next patient. Additionally, DSD can void the warranty as it specifically mentions with LIFEPAK. "LIFEPAK defibrillators comply with standards which require defibrillators to withstand defibrillation shocks from a second defibrillator connected to a patient. This testing does not include delivering simultaneous/sequential or overlapping 360J defibrillation shocks from two LIFEPAK defibrillators. There are no design and/or safety standards for use of external defibrillators to perform double sequential defibrillation. We cannot guarantee the reliability of functionality of devices subject to this off-label use. Product warranty cannot legally cover damage to LIFEPAK defibrillators which occurs as a result of performing an off-label use." This quote is from Gerstein et al in a 2017 Annals of Emergency Medicine paper. As implied above, it urges that both cost and patient safety must be considered with DSD. Given the lack of strong evidence to support the use of DSD, this may be another therapy to wait on until further evidence supports its use. For those who are considering using this method, consideration must be made as to other options such as adding esmolol, changing pad placement, or at least ensuring that if this equipment were to be damaged that there are replacement options. This could be more feasible in a hospital setting where there are usually multiple crash carts and another defibrillator can replace the one that is damaged. In the out-of-hospital setting though, this could take an entire ambulance out of service for an extended period of time. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed