
It is time for another EB Medicine special. The febrile young infant can be one of the scarier patients for a variety of reasons. They are so young they are unable to communicate, they have very real and serious pathogens that can have deadly consequences, and the family as well as other individuals taking care of the patient can be nervous or scared creating increased stress. In this post, we cover EB Medicine's recent article on this topic to better improve your practice.
For access to this article make sure to click this link. If you do not have a subscription yet with EB Medicine you will not be able to get the associated CME. However, check out the end of our show notes to learn how you can get access and at a great discount.
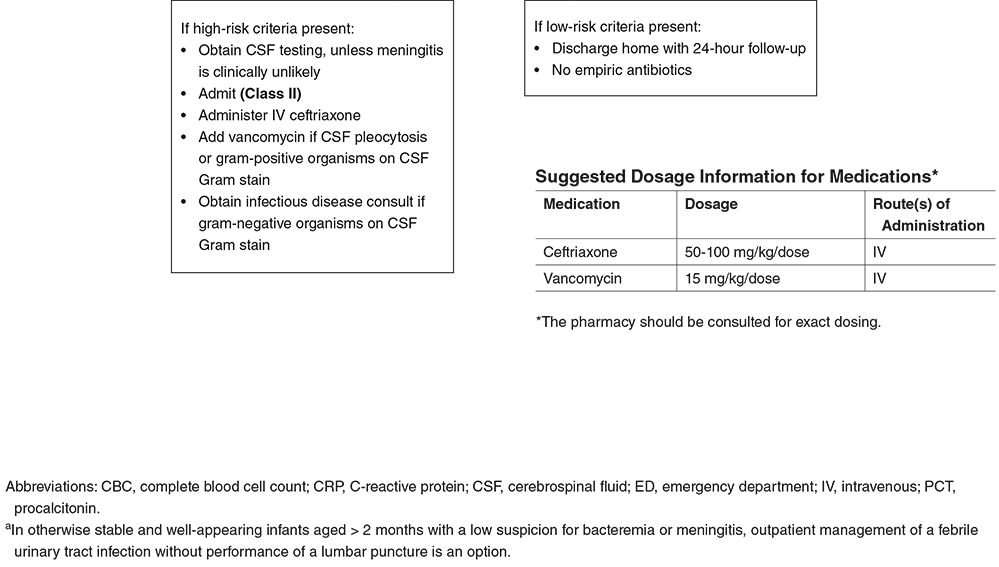
Sometimes the process to evaluate and treat the febrile young infant can seem very structured and methodical, especially at first glance. However, with different age ranges and a variety of data over time demonstrates that this is not totally the case. While the most structured and "routine" approach would be for neonates, there are even special considerations in these populations. We will break down some of the key highlights from the article to help guide us in our management based on the current evidence. First, why is this such a big deal? Due to their immature immune system, there is a high-risk for seriously bacterial infections (SBIs) and invasive bacterial infections (IBIs) in children aged 60-90 days or less. What makes it more challenging is the lack of social responsiveness (social smile), verbal cues, and that even in the well-appearing young infant they can still harbor serious infections. Additionally, there is a medico-legal component as the most common diagnosis in pediatric medical malpractice claims from the emergency department is bacterial meningitis. Key Definitions:
Causes for fever in well-appearing young infants:
Causes for fever in ill-appearing young infants:
The diagnosis of HSV can be rather challenging. Its presentation can vary depending on if it involves skin and mucous membranes, the central nervous system, or it is disseminated. EB Medicine has a great table to help break down the complexities. 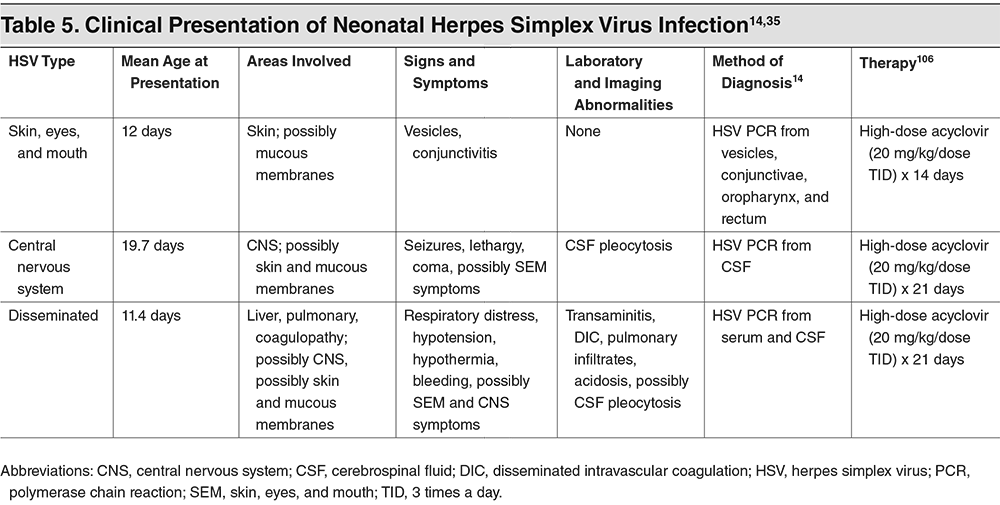
The history and physical is a vital component to our evaluation in addition to lab findings:
There are a variety of risk-stratification tools with varying types of data and suggestions. The most common along with their year of publication are the Boston Criteria (1992), Philadelphia Criteria (1993), Rochester Criteria (1994), Step-by-Step (2016), and PECARN (2019). The last three have MDCalc breakdowns to remind us of the cutoffs and criteria. It is also important to know that the last one, PECARN (Pediatric Emergency Care Applied Research Network) has not yet been externally validated and should currently be used only in infants aged 29-60 days. This is due to elevated herpes meningoencephalitis risk and and limited numbers of episodes of bacterial meningitis in neonates. 
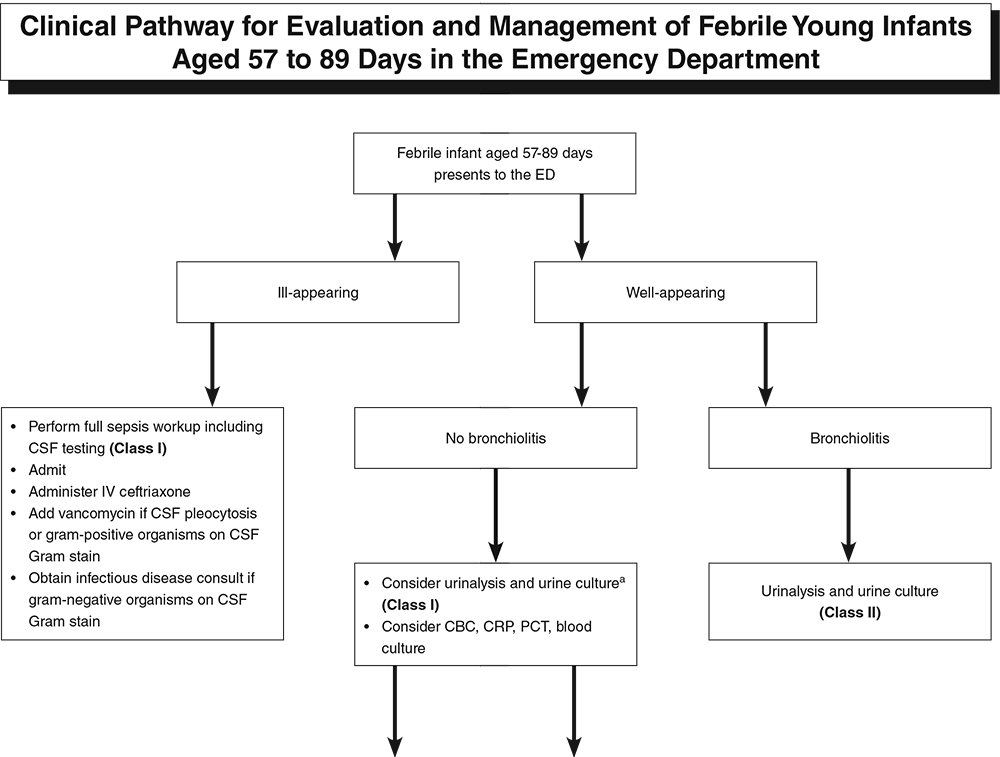
It is vital to remember no matter what method we use that we involve our pediatrician colleagues in the decision making process. In the case of those who are not as familiar with or comfortable in managing the febrile young infant to have additional support. This can be in the form of that pediatrician or even another one of our emergency medicine colleagues. Whatever the case, the more support we have the better.
Final Pearls from the Article:
Did you enjoy the content? Would you like to learn more about EB Medicine? Right now, you can get $50 OR MORE off a subscription with EB Medicine. Just click on this link and go to their website. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed