 Examining the gallbladder on ultrasound is not a particularly difficult skill. However, the rest of the biliary exam on point of care ultrasound (POCUS) can be both challenging and time consuming. Sometimes, the common bile duct (CBD) is not able to be positively identified. This has led to questioning the importance of this particular component of the exam. We will review some of the recent evidence in this post. It is worth remembering that biliary pathology is the third most common cause of abdominal pain that is seen in the emergency department. Evidence has demonstrated that no combination of clinical signs and laboratory testing are sufficient in the diagnosis and imaging is necessary. A systematic review from 2011 demonstrated that POCUS performed in the ED can be effective in detecting choledocholithiasis and cholecystitis. It can also help reduce the length of stay as a result. Biliary POCUS can help identify the following five pathological findings:
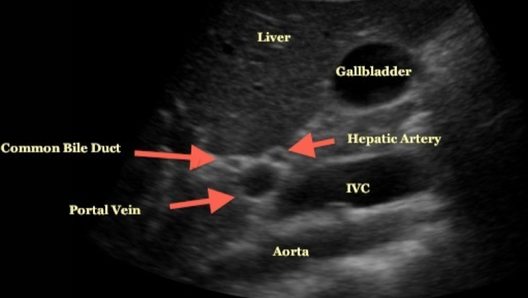
The CBD is the most difficult portion to identify and is assisted with identification of the portal triad (consisting of the portal vein, CBD, and hepatic artery) by seeing the “Mickey Mouse” sign often adjacent to the gallbladder. An example of this is noted above. A tip to help find the CBD is to follow the main lobar fissure to the portal triad. Having the patient reposition themselves or taking a deeper breath can also help. Once identified, color Doppler can be used to identify and differentiate the portal vein, CBD, and hepatic artery. The CBD will lack color flow. For patients less than 60 years of age, an internal diameter >6mm is pathologic. Newer evidence has demonstrated that for every decade of life after age 60 to add 1mm for this cutoff. Post-cholecystectomy, a normal CBD can measure up to 1cm in diameter. Still need help figuring out how to do this exam? Check out the video below from 5 Min Sono.
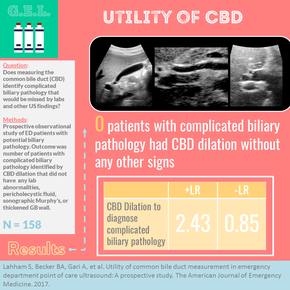
This finally leads us to our discussion for today. A 2017 paper discussed the utility of common bile duct measurement for POCUS in the emergency department. A detailed review of the paper can be found at the Ultrasound GEL Podcast which is where the graphic above came from. We are going to focus on the highlights and what it means for us in the emergency department. The study was performed at a single academic institution in a prospective, observational style. Patients had both laboratory studies as well as biliary POCUS. The gold standard was the diagnosis from the ED or hospital discharge. This could include further testing by ERCP or surgical pathology. Patients were also contacted two weeks after the visit and then monthly for a year if they were not successfully reached. Only at that point would they be excluded from the study. A big benefit was that this study was performed by resident, fellow, and attending physicians (not just one group) and all had completed at least an hour of didactic training but three hours of hands-on scanning. They were looking for CBD dilation as described above as well as wall thickness >3mm, pericholecystic fluid, or a positive sonographic Murphy's sign. An abnormal CBD was visualized 12.7% of the time and the CBD was not identified 4.4% of the time. Nearly 80% of patients had abnormal labs and nearly 75% had an abnormal POCUS exam. Gallstones were identified a little less than half of the time and a dilated CBD was identified just under a quarter of the time. Only two cases (1.3%) had complicated biliary pathology without laboratory or POCUS abnormality. They did not have CBD dilation either. Only two patients with CBD dilation (10% of cases) did not have at least one lab abnormality or abnormal POCUS finding outside of gallstones. In both cases it appears they only had uncomplicated cholecystitis. The only patient without a visualized CBD that had complicated biliary pathology was actually pancreatitis and they did have an elevated lipase. Almost 10% of the time when a dilated CBD was found did the patinet has uncomplicated cholelithiasis or a non-biliary diagnosis. This leads to a sensitivity of 23.7% and a specificity of 90.3%. There were some limitations given that these findings were not compared to a standard or expert overview, patients did not all receive a definitive study, there were no cases of cholangitis or malignancy, and these patients had an overall lower BMI than we expect from many of out patients (average of 28). However, this was overall a good study. While the CBD is beneficial to find when possible, it does not appear to contribute to diagnosing complicated biliary pathology (at least in this study). Other interesting findings were that the wall thickening was the most common abnormal findings and gallstones were only seen in about half of the cases. It truly is important that we look at the complete picture when performing biliary POCUS. Did you enjoy the content? Do you want to learn more about biliary ultrasound and other types of POCUS exams? Check out Practical POCUS! They have some upcoming courses and it can be a great way to use your CME funds before the end of the year. One option they include is to package their CME course with a Butterfly iQ. Make sure to check out their website to learn more. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||||
 RSS Feed
RSS Feed