
Both rashes and fevers are very common complaints in the emergency department. However, the challenge becomes very real distinguishing the serious to the more benign. Fortunately, EB Medicine has once again come to help make this challenging topic a little easier to understand. We review some of the highlights from their article in this post.
For access to this article make sure to click this link. If you do not have a subscription yet with EB Medicine you will not be able to get the associated CME. However, check out the end of our show notes to learn how you can get access and at a great discount.
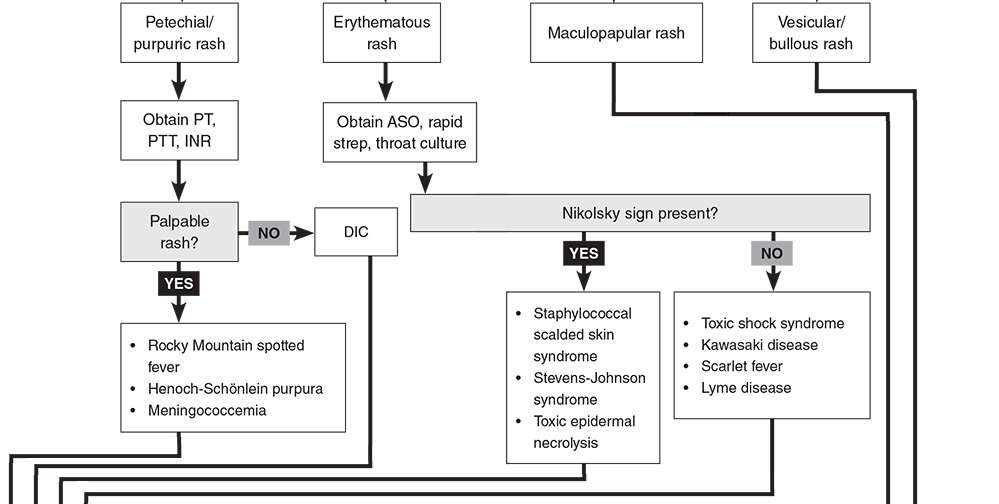
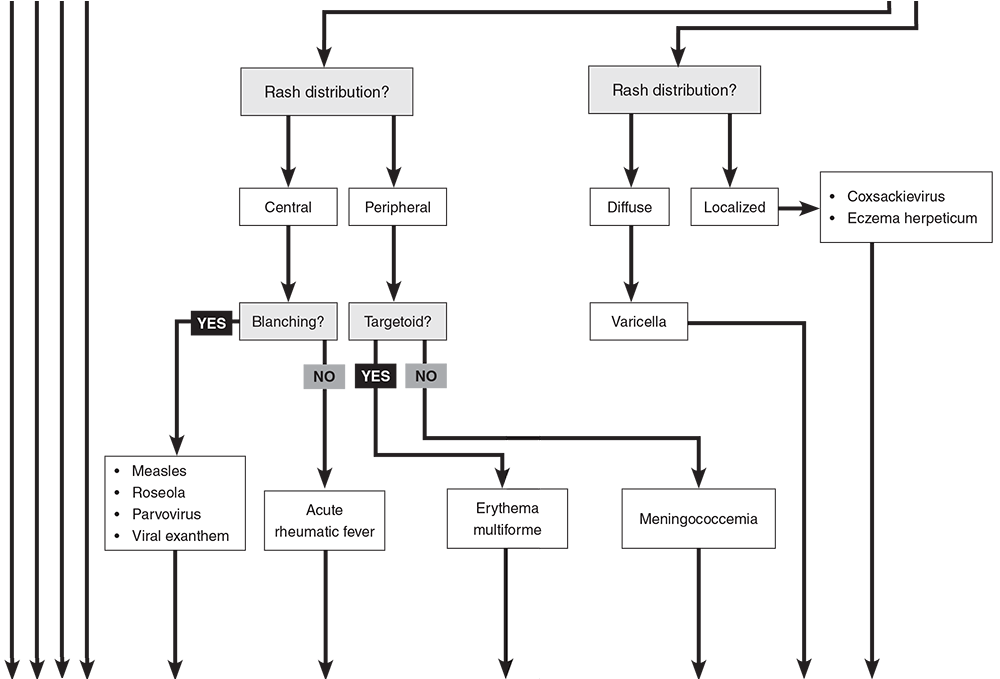
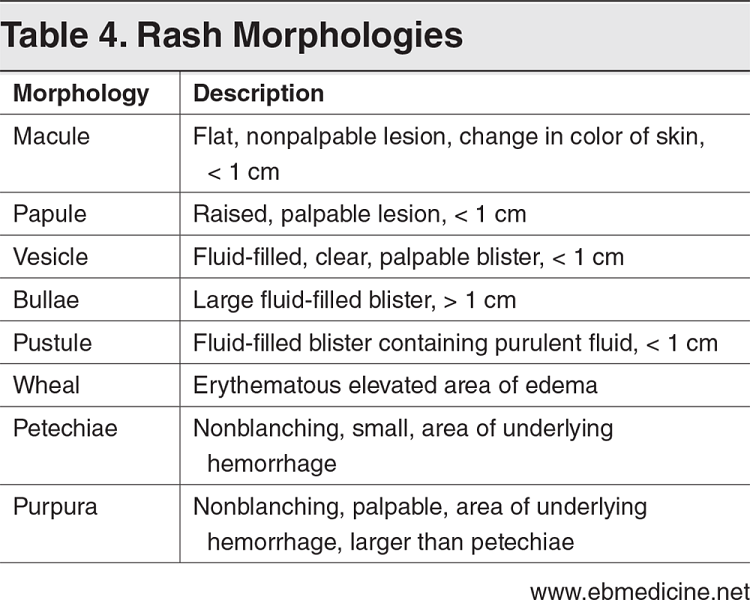
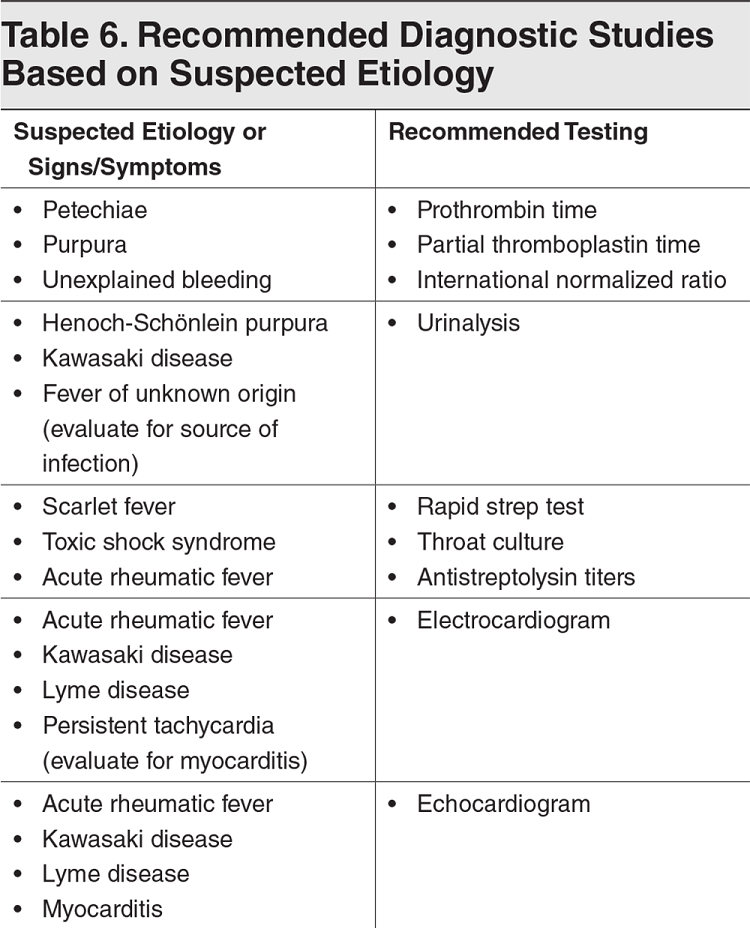
Overview The single most common chief complaint in the emergency department for children less than 15 years of age is fever and the fifth most common is rash. While many conditions are benign, there are some very serious ones that carry significant morbidity and mortality. Fortunately, many of our decisions can be made with a strong history and physical exam.By doing this properly, we can help identify them earlier and provide better care. We can even help with public health concerns such as varicella, measles, and rubella. Many viruses can present with a nonspecific exanthema with the maculopapular/morbilliform being the most common. The characteristics of the rash is usually the first step to help develop a differential diagnosis. While the EB Medicine article was great at reviewing many of the key rashes and their pathology in detail, we will focus on the distinguishing highlights and some key pearls. It is worth noting that the article did not discuss endemic diseases such as mosquito-borne and tick-borne illnesses but they should be kept in the differential if the history is suggestive of such etiologies. Additionally, this does not discuss other causes of rashes such as drug reactions. History When it comes to the history, determining a timeline is key. Did the rash or the fever come first? Has the fever resolved? When and for how long have both been present? What other symptoms are present? We must also consider the time of year, region, and recent travel history. Make sure to ask about medication use, recent vaccinations, and sick contacts. The vaccination status is also vital as vaccine-preventable diseases such as measles, varicella, and rubella have classic rashes and are more common in those not vaccinated. Due to anti-vaccination movements, they are also making a comeback. Physical Exam The physical exam is vital starting at the appearance of the child. An active, happy, and playful child can be reassuring for a more likely benign etiology. When examining the skin, it is important to accurately describe the findings. Check Table 4 below for a nice description of rash morphologies. Check the major distribution of the rash, if the rash involves the palms of the hands and soles of the feet, if the rash blanches, if their is mucous membrane involvement (including mouth, conjunctiva, and genitals), and if there is the presence of Nikolsky's sign. Nikolsky sign is described as the extension of peeling or blistering skin caused by separation of the layers of skin when firm, sliding pressure is applied. Nikolsky sign, non-blanchable rashes, and petechial/purpuric rashes are generally more concerning for serious pathology. However,the exclusion of these findings does not rule out serious etiologies. Other important characteristics on physical examination that can aid in the diagnosis includes lymphadenopathy, abdominal pain, arthritis, cardiac murmurs, and cardiac rubs. Splenomegaly can also be a helpful indicator when identified. Perform a neurological exam to identify focal deficits, chorea, and other abnormalities when rheumatic fever, Lyme disease, or meningitis are considered. Diagnostic Studies Lab testing is not always necessary. In many cases the history and physical will lead to the diagnosis. However, certain studies should be considered based on the suspected etiology or the signs and symptoms present. Check Table 6 below for more details. Petechial/Purpuric Rashes We will now briefly review some of the key aspects to the rashes described below in the clinical pathway created by EB Medicine. Purpura are caused by bleeding into the skin or mucosa from small vessels. This can be found in potentially life-threatening meningococcal disease. The cardinal sign of purpura is that it does not blanch with pressure. Small petechiae may also be present. Meningococcal disease must be considered in any patient with a patechial and/or purpuric rash given its rapid progression and high risk of complications including death. Henoch-Schönlein purpura (HSP) is the most common pediatric vasculitis and cutaneous manifestations occur in all cases. Necrosis of small blood vessels results in a nonthrombocytopenic purpura and is the initial feature on presentation in 75% of cases. It is characteristically described as a symmetric, dark red or purple, nonblanching, palpable exanthem. During the first 24 hours the rash may have a maculopapular or urticarial appearance that evolves. The rash may appear as deep bruises or bullous or hemorrhagic lesions. Erythematous Rashes Kawasaki disease is an acute, multisystem vasculitis that can lead to heart disease with the secondary complication of coronary artery aneurysm which is seen in 20-25% of untreated cases. The rash it typically a widespread targetoid, morbilliform, or macular exanthema. Unlike the others described so far, its diagnosis is based on clinical criteria. Check MDCalc for the diagnostic criteria. Scarlet fever is most commonly seen between 5 and 15 years of age. The classic description is a scarlatiniform "sandpaper" rash that is blanching and maculopapular. It spares the palms and soles. Throat culture is the gold standard of testing but a rapid antigen test can provide a more immediate answer. Toxic shock syndrome is easily recognizable and very serious. Hallmarks are fever, hypotension, and rash with multiorgan failure often being seen. Desquamation of the hands and feet may occur. Erythroderma is a diffuse, red, and macular rash that resembles a sunburn. Mucous membranes can be involved. Part of the examination should be a search for a nidus of infection such as retained tampon which should be promptly removed. Even subtle wounds can be a source of infection. Nikolsky sign distinguishes staphylococcal scalded skin syndrome (SSSS) from the others described in this section. The separation of the epidermis causes a painful, sunburn-like rash and development of bullae (large, fragile, fluid-filled blisters). When the bullae burst they slough in a sheet-like manner leaving a moist and reddish area on the surface. Maculopapular Rashes Measles is highly contagious and begins as a viral prodrome. Koplik spots may develop which are small white, gray, or bluish spots with an erythematous base that develop along the buccal mucosa and are pathognomonic for measles. The morbilliform rash usually appears 3-4 days after symptoms begin starting on the head and moving to the torso then extremities. Confluent areas may appear and the rash will fade around the fifth day after it develops. Patients are contagious for this entire period. Many secondary complications may occur such as hearing loss, blindness, or death often secondary to pneumonia. Uniquely, Vitamin A supplementation can help in improving outcomes. Erythema infectiosum (Fifth Disease) has the classic exanthema characterized by the "slapped cheek" appearance with the perioral and nasal folds being spared. By the time the rash appears, the patient is no longer contagious. However, isolation is important as infection in a pregnant woman can lead to severe hydrops fetalis or intrauterine fetal death. This is considered one of the TORCH diseases. Roseola has the hallmark of rash appearing after the fever resolves, usually 12-24 hours later and has small, erythematous, blanching papules often starting on the trunk. It is known to increase the risk of febrile seizures which occurs in up to 15% of those infected. Acute rhematic fever (ARF) occurs after group A streptococcal infection usually within 2-4 weeks and can occur even when it was treated. Clinical manifestations include carditis, arthritis, chorea, and subcutaneous nodules and erythema marginatum. The nodules are firm but painless and found on extensor surfaces. Erythema marginatum is a pink rash with pale centers and rounded or serpiginous margins. Those suspected to have it should be admitted for further evaluation. Vesicular/Bullous Rashes Varicella is described often as a "dew drop on a rose petal" in appearance. Skin infections may occur from the scratching. More serious infections such as pneumonia or CNS infection are far more rare but significant, especially in those immunocompromised. Hand, foot, and mouth disease (HFMD) has a brief prodromal stage with fever, sore throat, and refusal to eat or drink. Its characteristic rash are blister-like lesions to the hands and feet including the palms and soles. They may be tender on palpation. Oral lesions can be visualized and usually isolated to the posterior pharynx. Not all three areas may be involved. The most common complication is dehydration due to not wanting to drink but rarely CNS infections or cardiac complications like myocarditis may occur. Summary This is not meant to be an exhaustive review, but the information can be very beneficial in helping you identify the source of the rash and fever. Use the tables below to help you further. 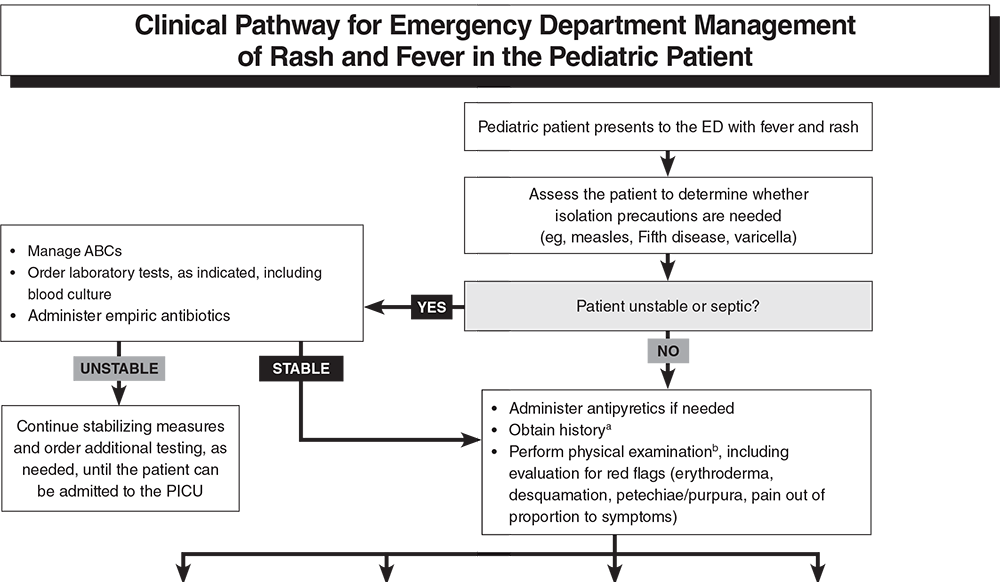
Obtain additional diagnostic testing, if needed, and determine disposition based on suspected etiology and other signs/symptoms (see Table 6 below).

Did you enjoy the content? Would you like to learn more about EB Medicine? Right now, you can get $50 OR MORE off a subscription with EB Medicine. Just click on this link and go to their website.
Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||||
 RSS Feed
RSS Feed