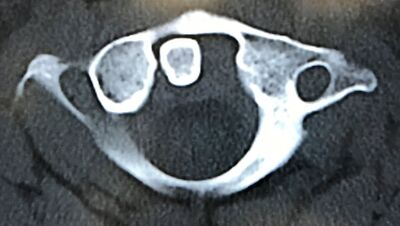
Injuries to the spine can occur both in blunt and penetrating trauma. They can also be with or without neurological deficits. For this reason, they should be considered in all patients with multiple injuries. In this podcast, Chip Lange and Mike Sharma review the pearls and pitfalls of this disease process.
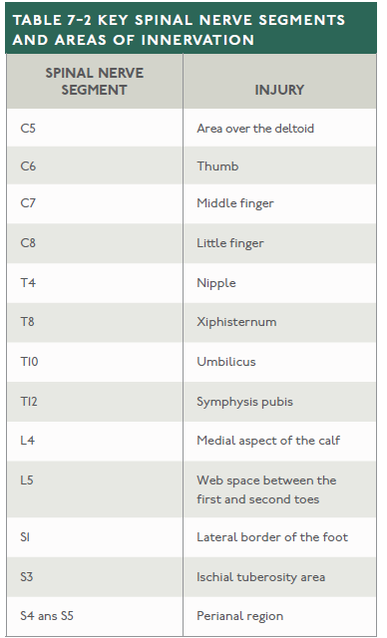
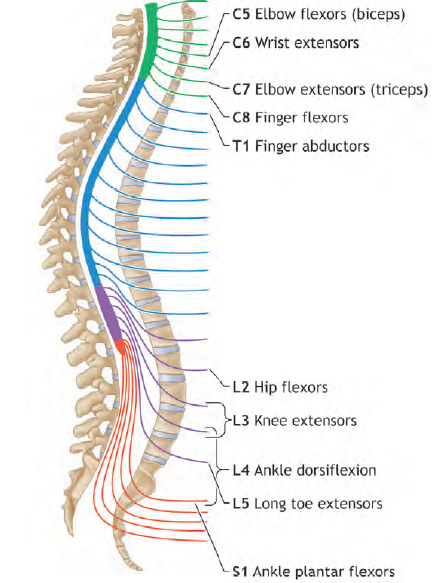
It is worth remembering key dermatomes (pictured left) and myotomes (pictured right) as seen in the two images below. Dermatomes are areas of skin innervated by the sensory axons within a particular segmental nerve root. Myotomes are essentially the equivalent for muscles but most muscles are innervated by more than one root (usually two).
Neurogenic shock results in the loss of vasomotor tone and sympathetic innervation to the heart. Injury to the cervical or upper thoracic spinal cord (T6 and above) can cause impairment of the descending sympathetic pathways. The resultant loss of vasomotor tone causes vasodilation of visceral and peripheral blood vessels, pooling of blood, and, consequently, hypotension.
Spinal shock refers to the flaccidity (loss of muscle tone) and loss of reflexes that occur immediately after spinal cord injury. After a period of time, spasticity ensues. Neurogenic shock and spinal shock were discussed recently on EMCrit and it is worth listening to that podcast by Scott Weingart. We also covered how there may be a benefit in trauma in Podcast #216. In general, vasopressin should at least be considered especially after volume resuscitation. We did cover spinal cord syndromes and there is some additional information in the infographic below that can be very helpful in understanding the differences. However, the website that it comes from is no longer functional. 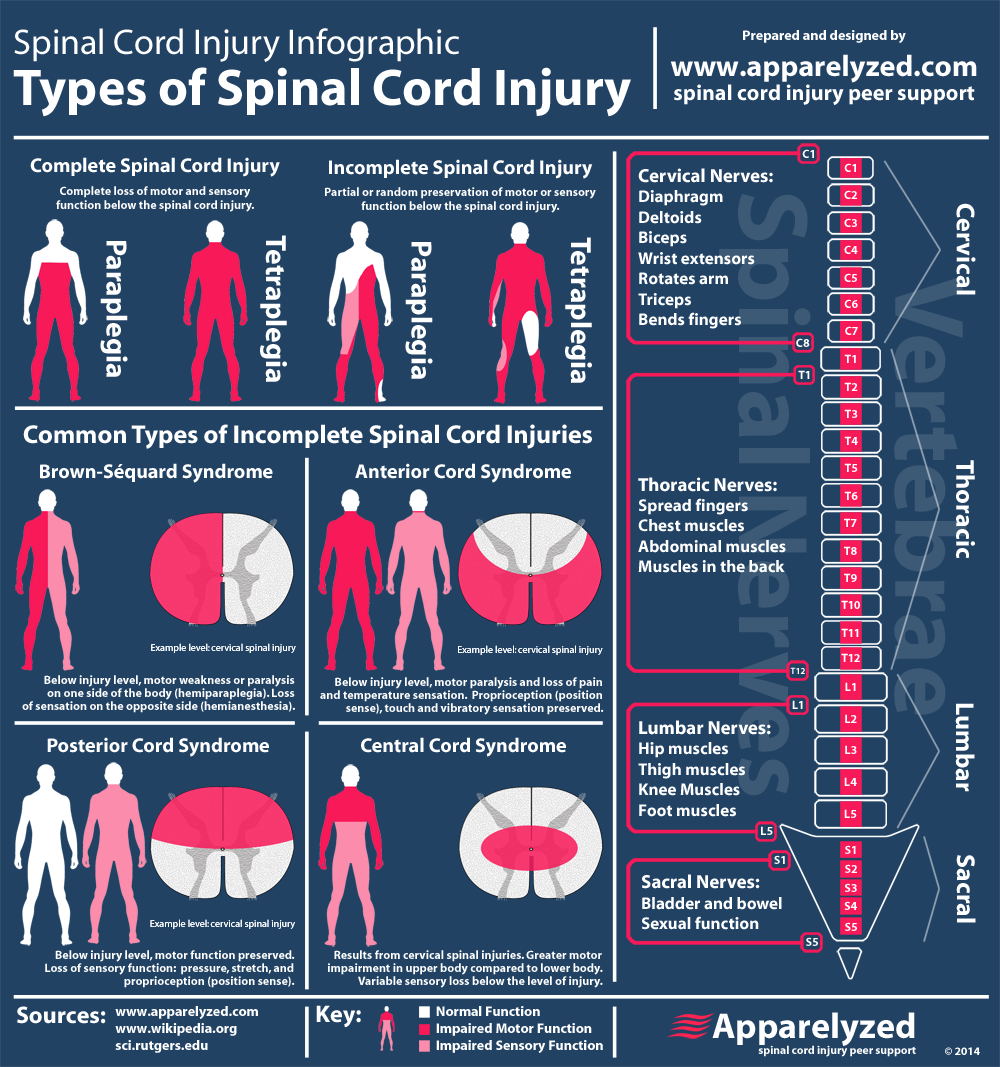
When it comes to evaluation, there is a way to help us risk stratify cervical spine injuries. However, the thoracic and lumbar portions of the spine do not benefit from rule out criteria. There are also certain injuries to watch for specifically as discussed in the podcast.
The Canadian C-Spine Rule (CCR) and the National Emergency X-Radiography Utilization Study (NEXUS) are widely used. The CCR is used more frequently now than the NEXUS criteria, but both are specifically mentioned in this ATLS chapter. Simple compression fractures are usually stable and often of the thoracic and lumbar spine are usually stable and often treated with a rigid brace. Burst fractures, Chance fractures, and fracture-dislocations are extremely unstable and nearly always require internal fixation. Chance fractures can be associated with retroperitoneal and abdominal visceral injuries. Given the narrow relation to the spinal cord and canal a the level of the thoracic spine means that fracture-dislocations (or subluxations) can commonly result in complete neurological deficits. Finally, thoracolumbar junction fractures (T11 through L1) are due to immobility of the thoracic spine compared with the lumbar spine and are often considered unstable due to their vulnerability to rotational movement so be careful in logrolling these patients. Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on Apple Podcasts. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
1 Comment
|
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||||
 RSS Feed
RSS Feed