
Kris Maday is back for another podcast which is also available at the PAINE Podcast this time to discuss complications of chemotherapy. We review some of the most common conditions that also possess a risk to be life threatening for those fighting cancer. Since chemotherapy is designed to kill rogue cancer cells (some by sniper, some by nuke), there is bound to be collateral damage. The detailed show notes provided are in large part from Kris Maday's review of the literature.
Therapeutic Index
This is the balance between toxic and therapeutic dosing of pharmacotherapeutic agents, and can be described as the relationship between underdosing (seeing no effect), effective dosing (achieving desired results), and overdosing (having toxic complications). Specifically, it is the difference between the toxic dose for 50% of the population and the effective dose for 50% of the population. 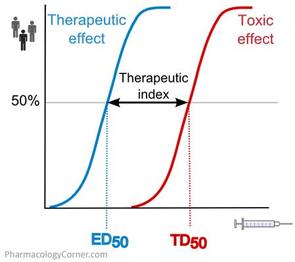
Myelosuppression
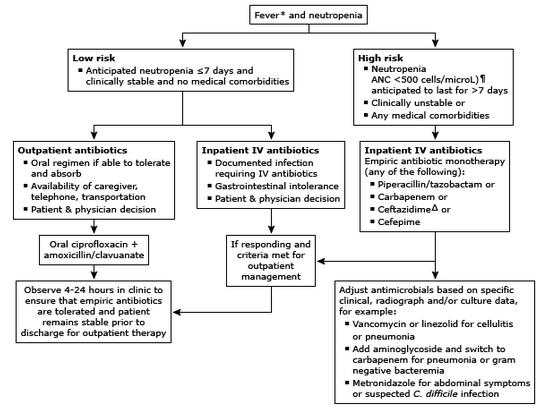
By definition, chemotherapy is designed to destroy mature, cancer cells, so it only makes sense that bone marrow suppression is affected. The most dreaded complication associated with myelosuppression is acquired neutropenia. This can occur anywhere from 2-6 weeks after chemotherapy and the only presenting sign that something is wrong is a febrile episode (>38oC). Definition of neutropenia is an absolute neutrophil count (ANC) < 1500 cells/microL. This can be automatically calculated by most labs, but it is calculated as follows: ANC = WBC x 10(%PMN + %Bands) Risk assessment is done via the Multinational Association for Supportive Care in Cancer (MASCC) index: 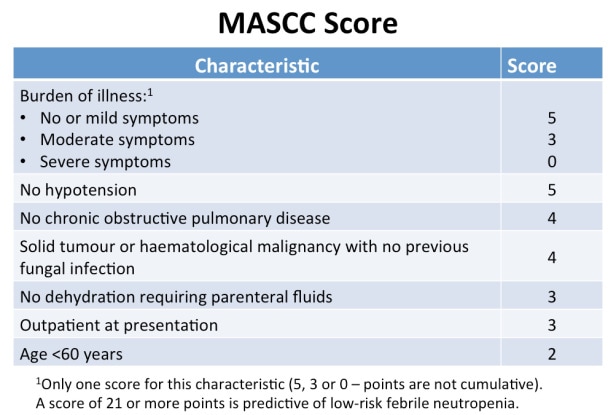
Nausea and Vomiting
N/V associated with chemotherapy can be acute (<24hr), delayed (>24hrs), or even anticipatory (prior to treatment). Chemoprophylaxis for N/V is based on risk and broken down into highly emetogenic, moderately emetogenic, low emetogenic, and minimally emetogenic therapies. 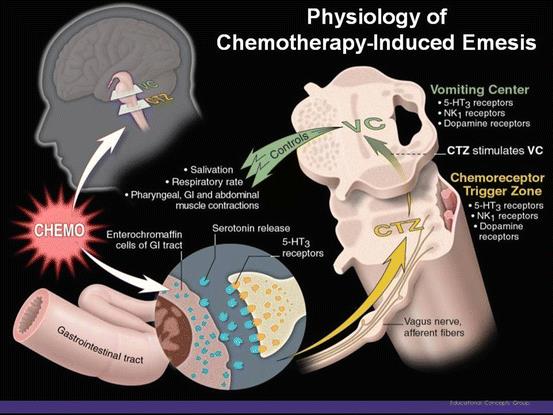
Mucositis
Profound inflammatory process of the mucous membranes and is characterized by: • Initiation of insult (chemo) • Upregulation/Generation of messenger signals and proinflammatory cytokines • Signaling and Amplification (Damage of tissue by cytokines is amplified via feedback loops) • Ulceration and inflammation • Healing Symptoms generally start to begin after day 7 and can range from mild inflammation to complete ulceration and inability to take anything PO. Epithelial sloughing after ulceration can produce the classic pseudomembane appearance. This desquamation can now lead to bacterial translocation in an already immunocompromised host. 
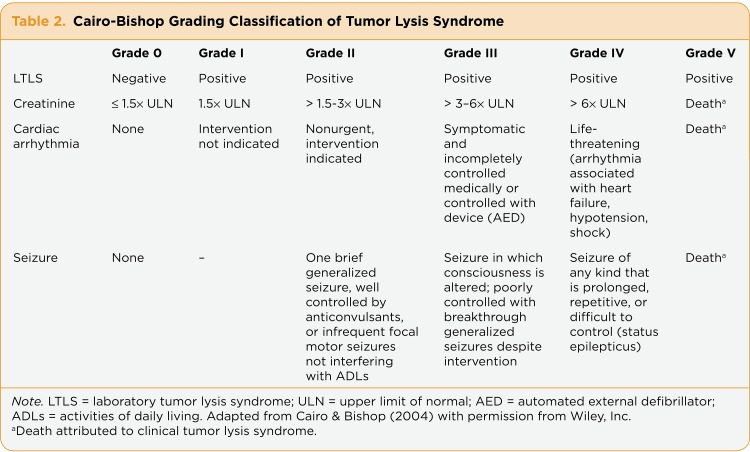
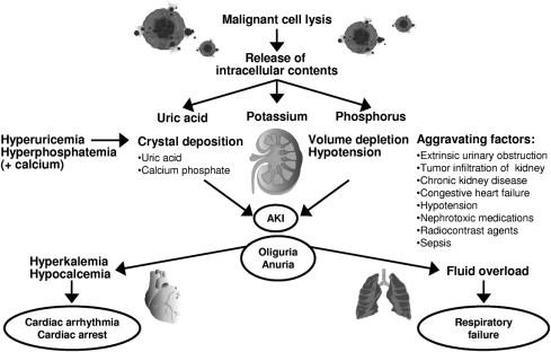
Tumor Lysis Syndrome
Occurs after massive tumor cell lysis (most commonly with high-grade lymphomas and ALL) and can cause the following biochemical abnormalities: • Hyperuricemia (Can cause uric acid nephropathy and AKI) • Hyperkalemia (From the lysis and intracellular distribution) • Hyperphosphatemia (Can cause calcium phosphate deposition in the renal tubules and precipitate AKI) • Hypocalcemia (Hyperphosphatemia causes significant hypocalcemia & can precipitate dysrhythmias) Diagnosis can be made with 2 or more laboratory abnormalities, or one laboratory abnormality and one clinical abnormality. Treatment is multitiered and consists of: • Fluid resuscitation • Electrolyte correction • Renal protection • Rasburicase – oxidizes uric acid 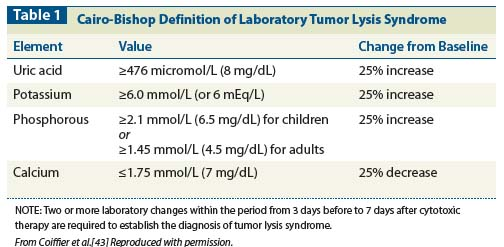
There is a lot to cover in a short time, but listen to the podcast for more details with its many pearls in the discussion. Also check out Kris Madays' post on the topic. Please let us know about any questions or comments you have in regards to the podcast. You can also reach us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
0 Comments
Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed