Happy Fourth of July! Today we are joined by Evidence Based Medicine (EBM) rock star Ken Milne who is known for the Skeptics' Guide to Emergency Medicine (SGEM) blog and podcast. He has been a major mentor to the TOTAL EM project and to celebrate our 50th podcast he agreed to join us for a detailed discussion on FOAMed and EBM. Both SGEM and TOTAL EM are part of the Free and Open Access to Medical Education (FOAMed) movement.
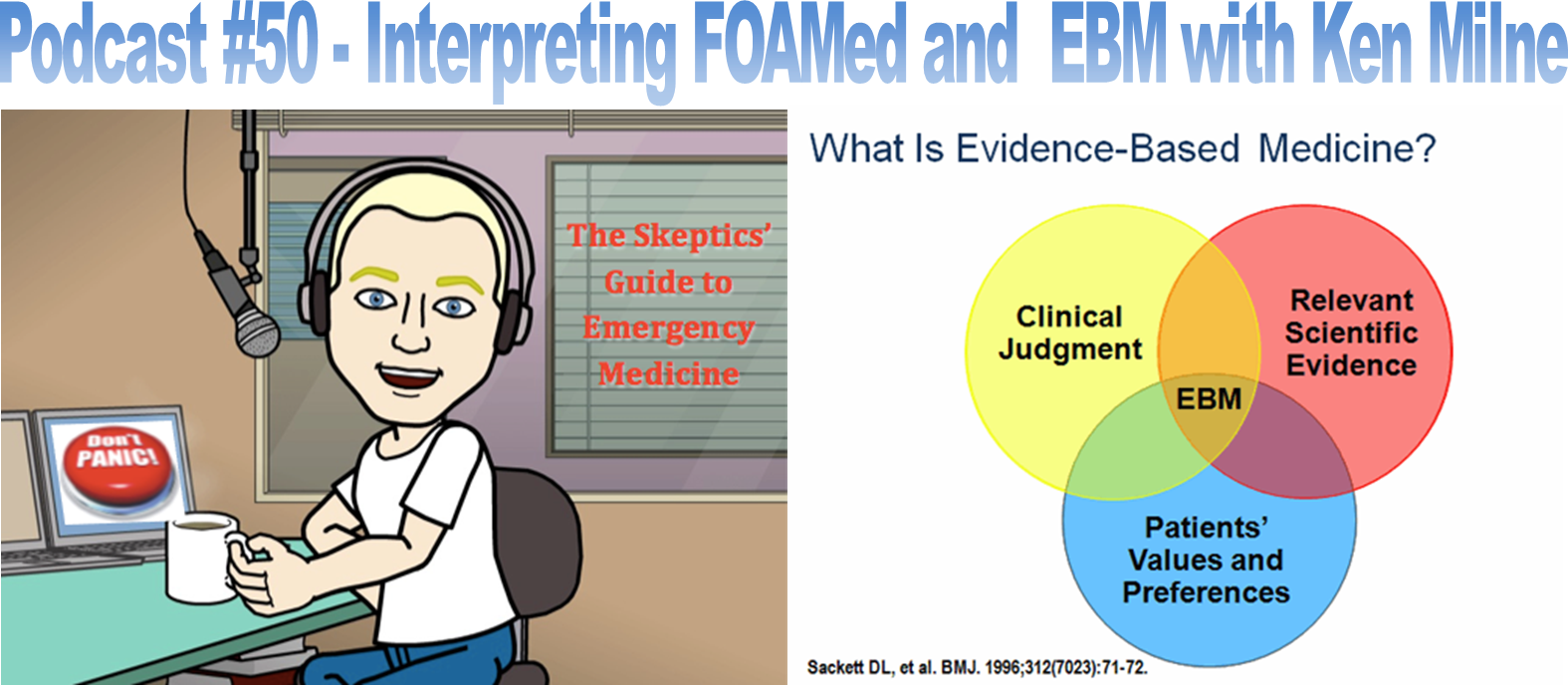
What is EBM? The answer is detailed in the podcast, but essentially it is a mix of three important aspects: patients' values and preferences, relevant scientific evidence, and clinical judgement. Remember that the scientific evidence is only one portion. It is always important to add clinical judgement for a particular scenario as well as the patient. The patient in front of us at a given time has their own values and preferences which we should follow to the best of our ability. Our judgement as to the situation and what we believe is best given the evidence all times into EBM. For that reason, EBM is much more complex than meets the eye.
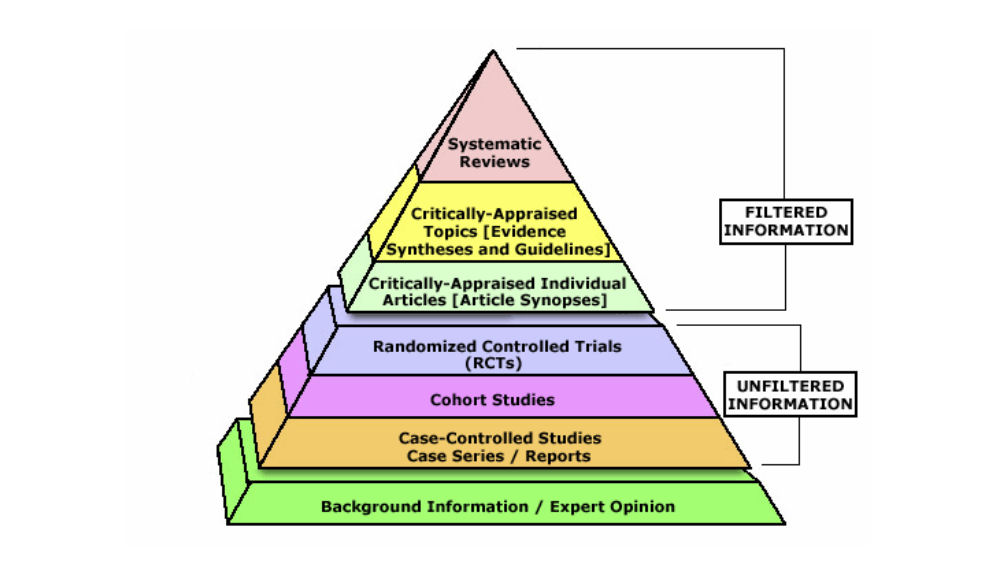
Above is a suggested hierarchy of evidence. Expert opinion is at the bottom and for a good reason: it is the least evidence based. Compared to other forms of evidence, it has the least scientific evidence. Many will recognize that RCTs are an important part of trials and often considered very high level. Although this is true in general, it is still not high in the hierarchy. Filtered information is considered higher with analyses of multiple papers being more helpful. The reason why is that evidence from a series of papers (and not just one such as with a single RCT), is far more beneficial for comparison. Systematic reviews are in many ways considered to be at the top of the pyramid. We often see this play out in ways such as with the high validity often seen with Cochrane reviews. However, we must again think about the grand scheme of things with out patients and not forget the importance of evidence based medicine being also about the patient and clinical judgement.
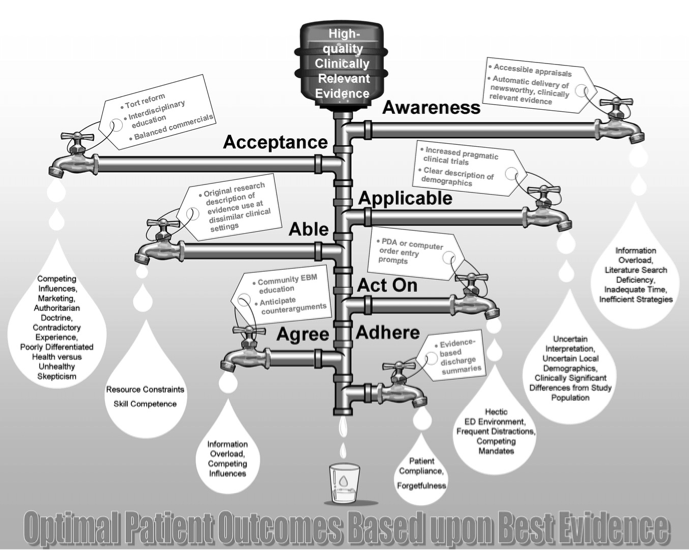
People often ask about why more evidence is not actually translated to the bedside. For example, practice may change considerably from one hospital to another or even from one provider to another in the same department. This is often due to issues with knowledge translation. FOAMed has been a major help with cutting down the time it takes for knowledge to reach those treating patients, but it is often more complex than simply releasing information. There is so much out there that there is no simple fix. The above diagram demonstrates the concept of the "leaky pipe" and explains ways in which knowledge translation is delayed. It is worth learning this as awareness (just as specified above), is often the first and largest obstacle in EBM.
Remember, EBM is a process. Someone does not just adopt it overnight. At the same time, we have all been using EBM to a certain degree. What you learned in school can be considered EBM, but we are talking about upping the game to another tier. Better understand and interpret the information out there by using great resources and the EBM Venn diagram shown above. Also, remember what Joe Lex said about staying up to date on medical knowledge:
Ken Milne also has his five take-home points for today:
How do you feel about FOAMed and EBM? Obviously, by listening and reading you at least consider information being delivered this way. Do you have preferences and ideas when you are going through this material? Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on iTunes. If you have any questions you can also comment below, email at [email protected], or send a message from the page. Please check our bandwidth sponsor, FunnyRx, too. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
2 Comments
|
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||
 RSS Feed
RSS Feed