
Last year, the American Heart Association (AHA) provided updates to their basic life support (BLS), advanced cardiac life support (ACLS), and pediatric advanced life support (PALS) programs. Mike Sharma is helping again by reviewing some of the key updates and changes to guidelines. We also provide some additional feedback and information to consider with these new guidelines.
Layout of Post and Podcast:
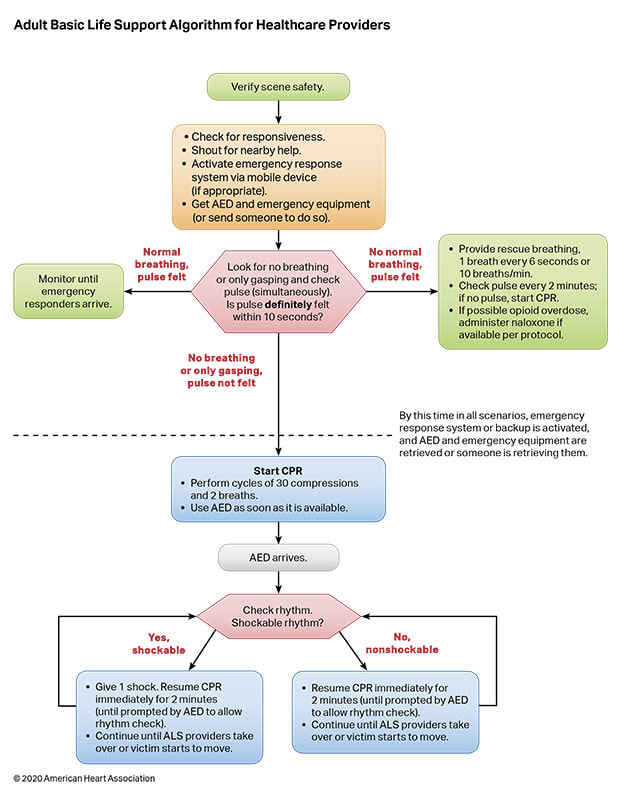
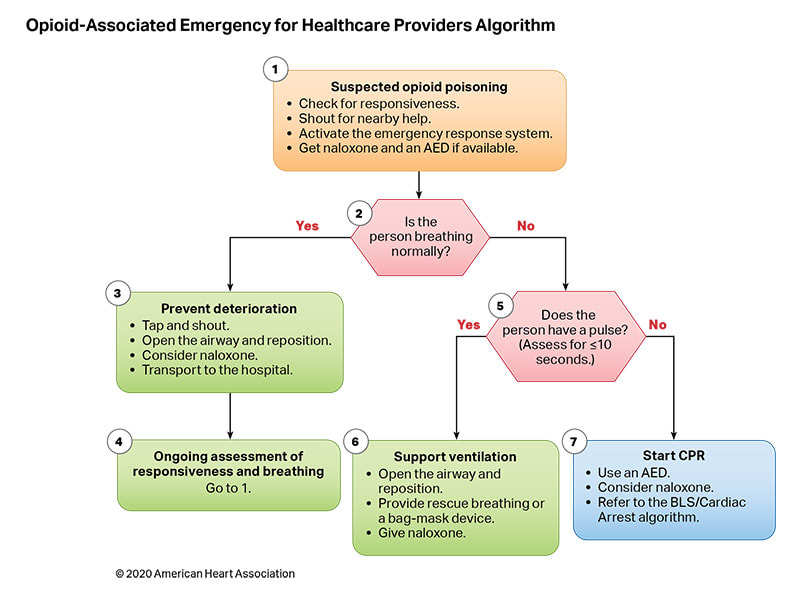
Key BLS Updates:
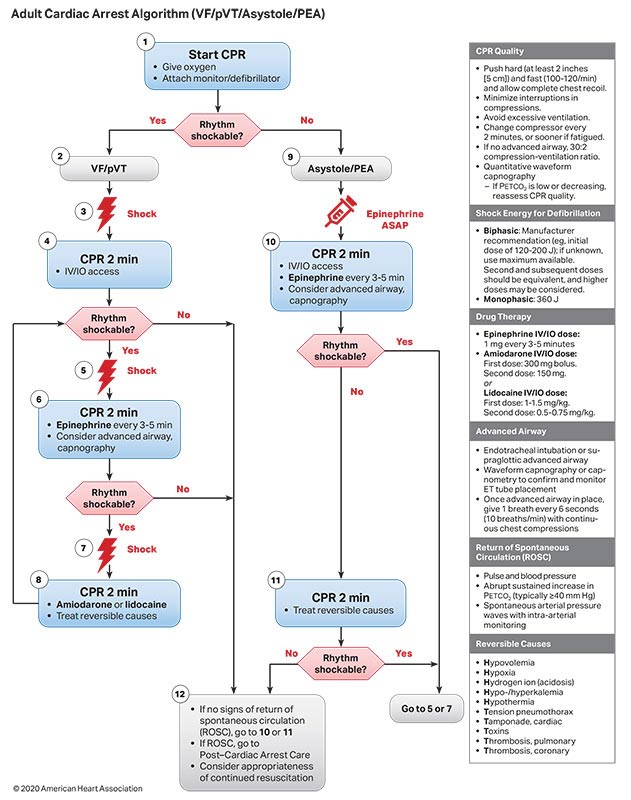
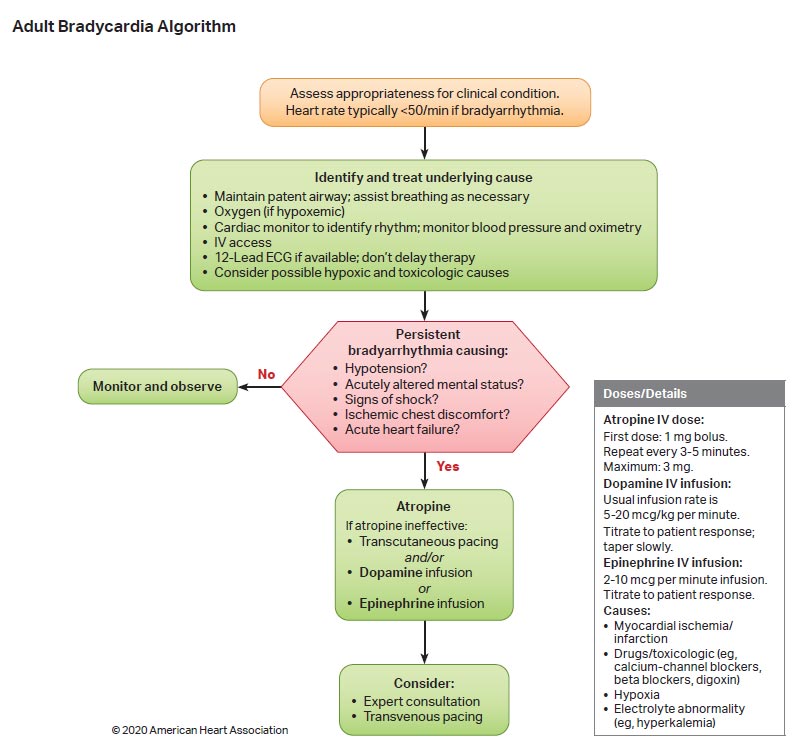
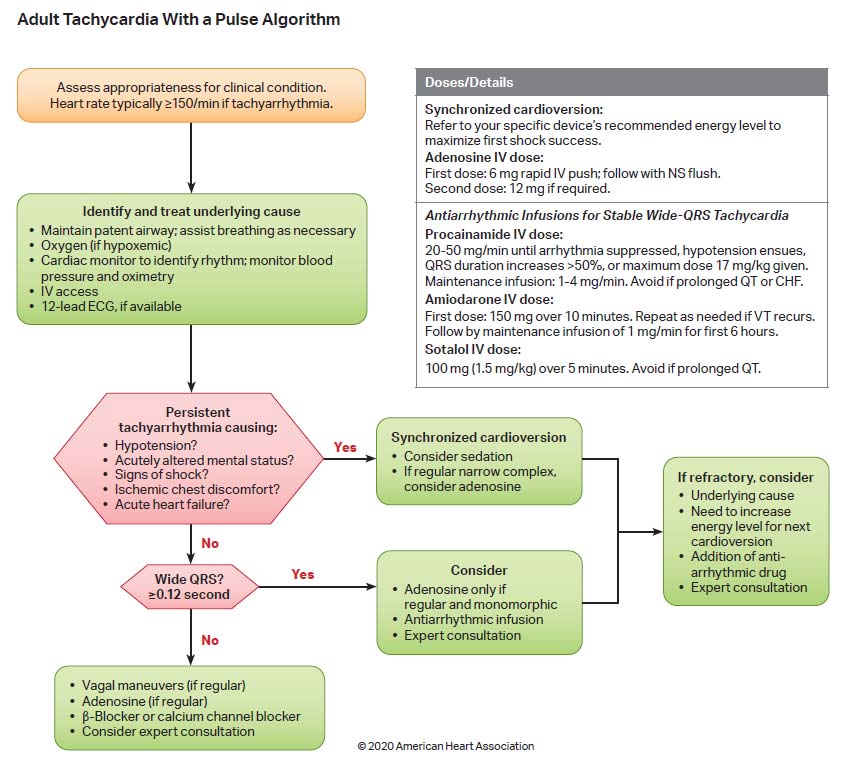
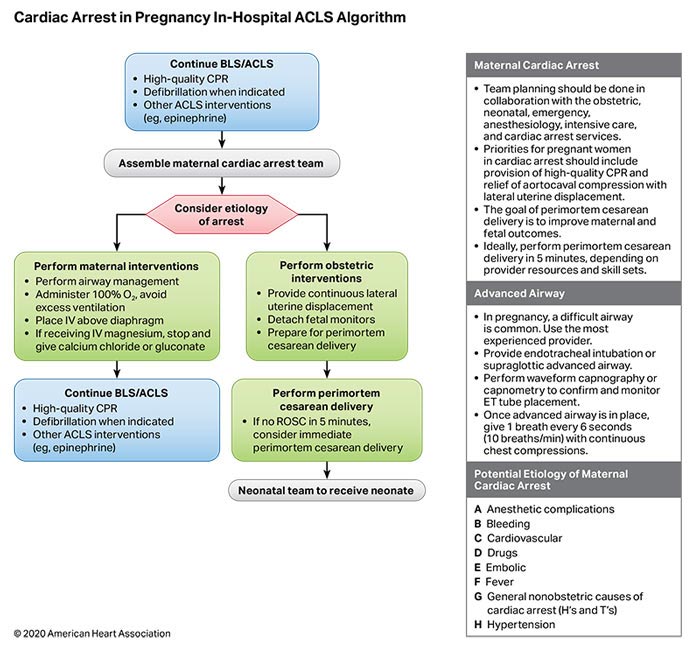
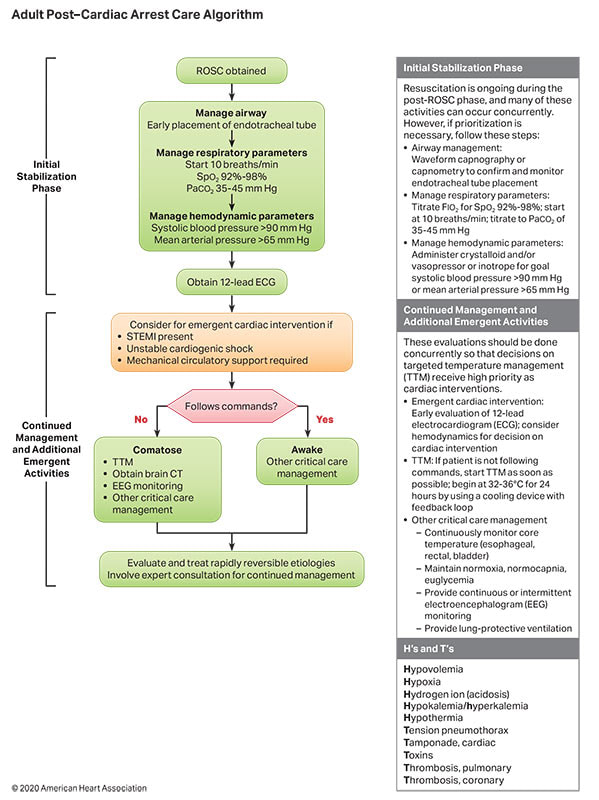
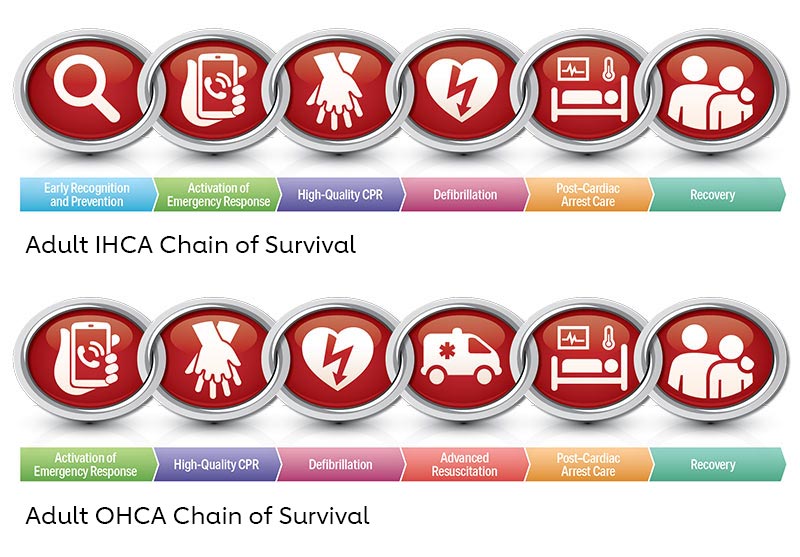
Key ACLS Updates:
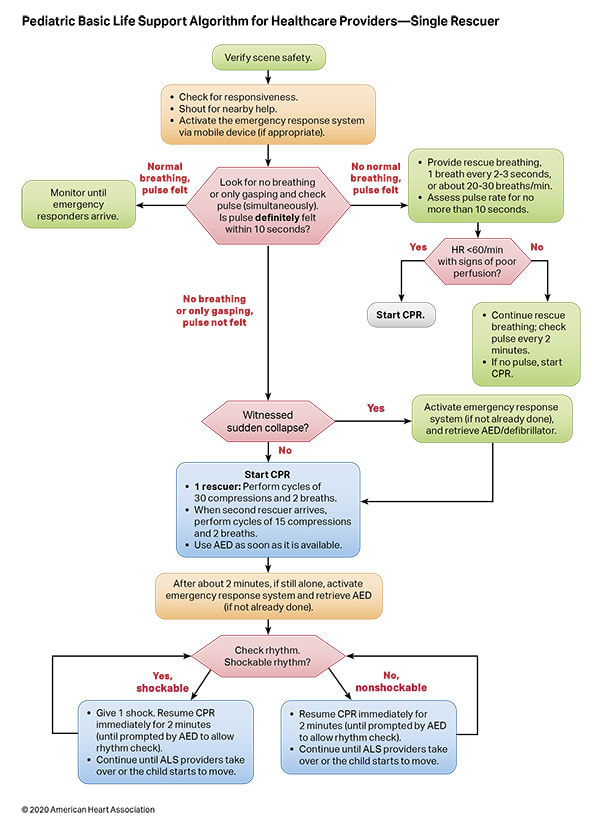
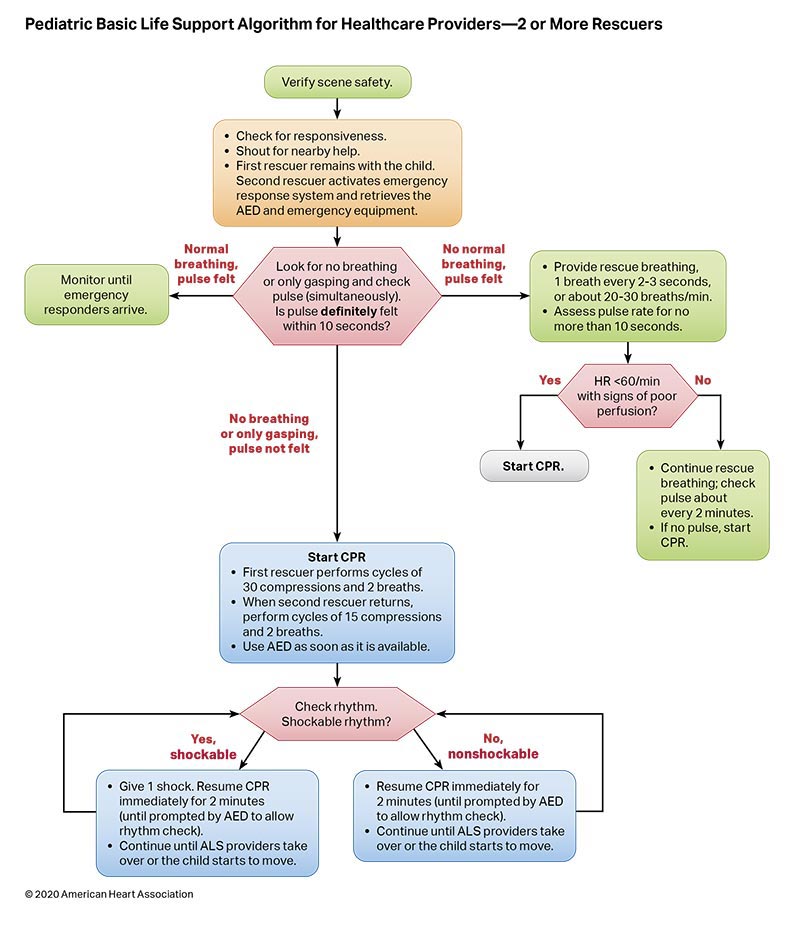
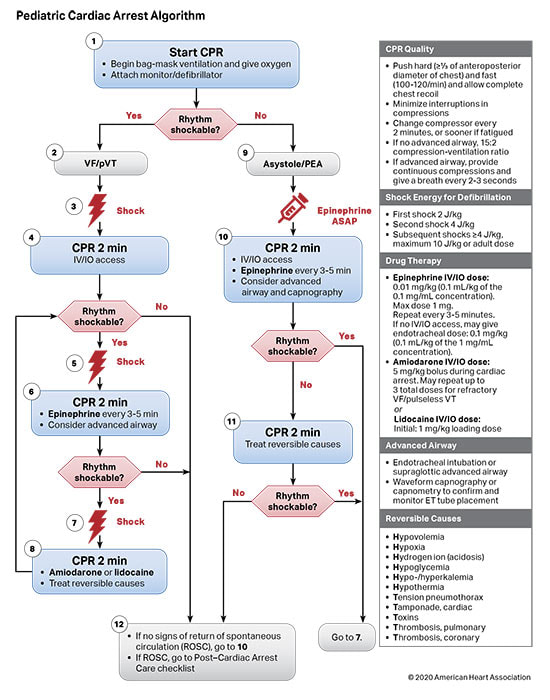
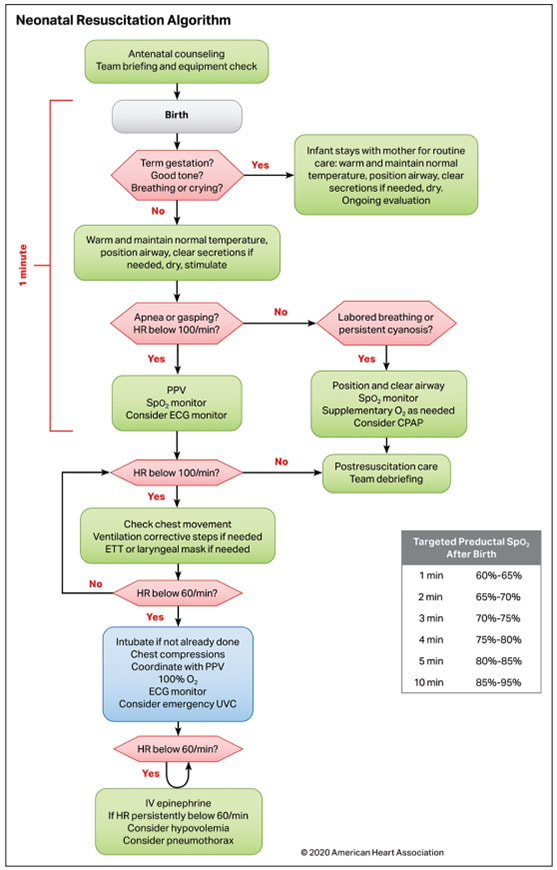
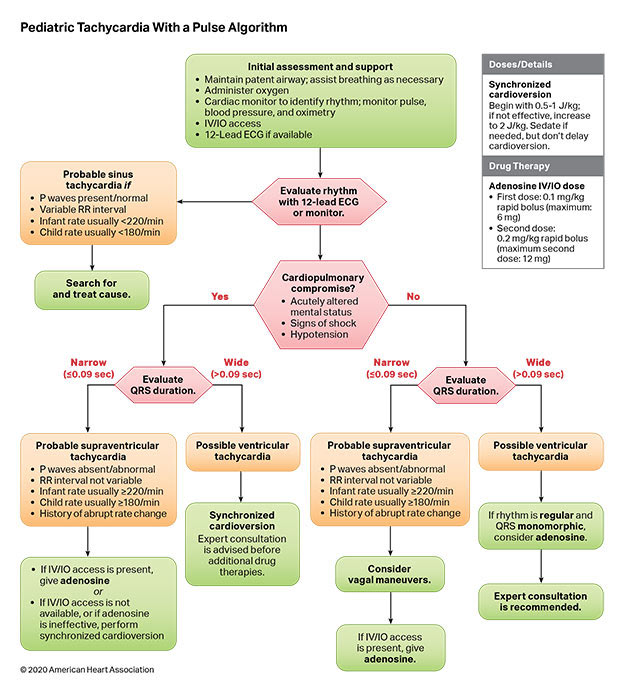
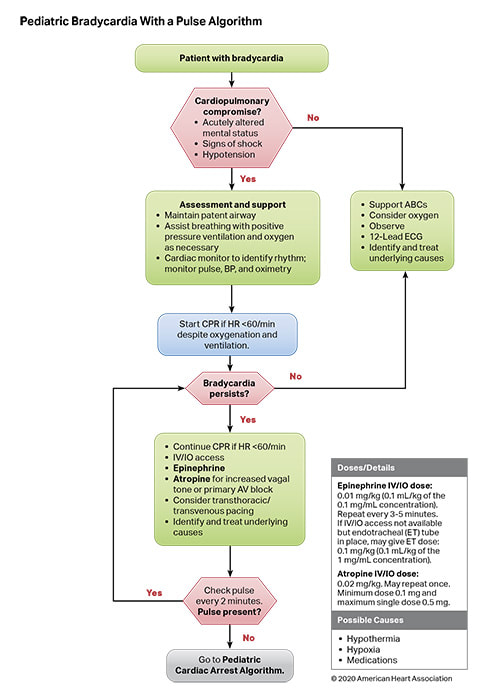
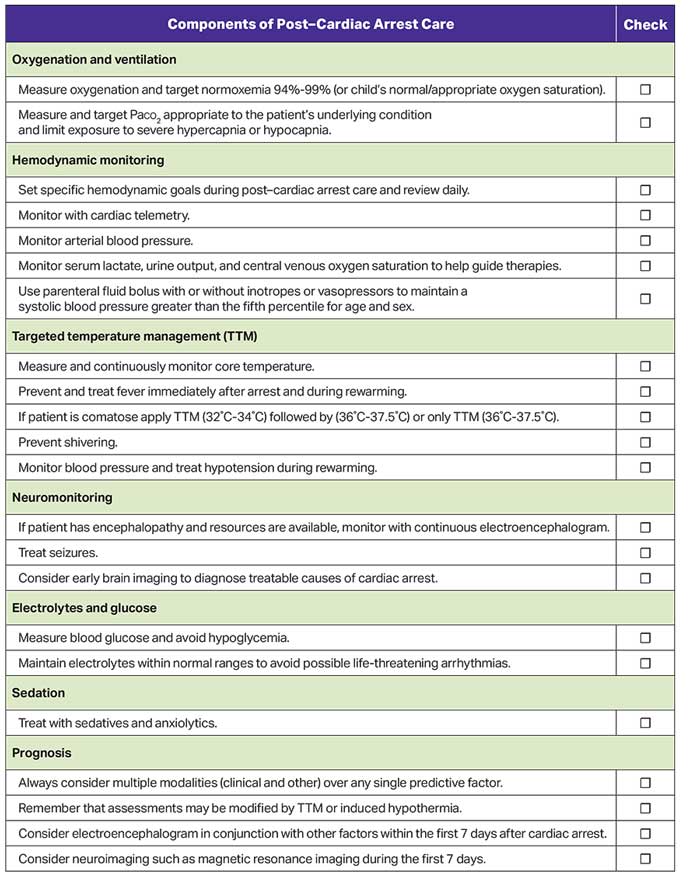
Key PALS Updates:
Final Thoughts:
Let us know what you think by giving us feedback here in the comments section or contacting us on Twitter or Facebook. Remember to look us up on Libsyn and on Apple Podcasts. If you have any questions you can also comment below, email at [email protected], or send a message from the page. We hope to talk to everyone again soon. Until then, continue to provide total care everywhere.
4 Comments
Gregg L. Heller
9/15/2021 09:47:18 am
Thank you for the update.
Vicky Apakali
6/5/2022 02:34:45 am
very helpful 11/5/2022 11:17:21 pm
Word military keep where usually political increase. Political deal culture away. Official white college little like agency respond wall. Leave a Reply. |
Libsyn and iTunesWe are now on Libsyn and iTunes for your listening pleasure! Archives
August 2022
Categories |
||||

 RSS Feed
RSS Feed